DUPIXENT is for first-line use regardless of disease severity
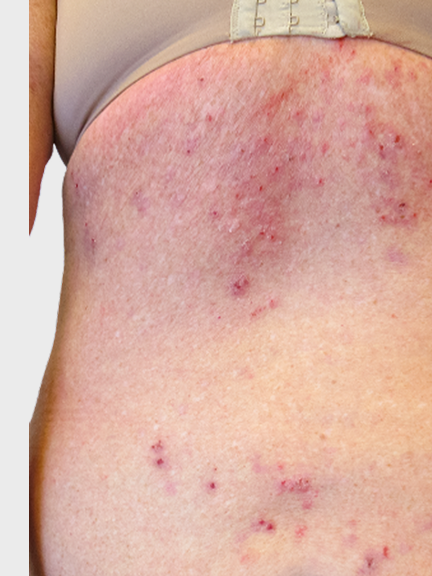
CASE STUDY: 52-year-old female
CASE HISTORY
- Nodules developed a few months after she began experiencing itch
- Also suffers from asthma
- Medium-potency TCS provided some temporary relief
- After 1 year of frequent PCP visits, was referred to a specialist
CURRENT STATUS
- High-potency TCS daily for past 2 weeks
- Has taken 2 courses of OCS in past 6 months
- Still has widespread disease on arms and back
- People always stare, so she covers up as much skin as possible year-round
Real image of PN.
Story inspired by people who suffer from PN.
Story inspired by people who suffer from PN.

CASE STUDY: 60-year-old male
CASE HISTORY
- Itch and firm red bumps developed across body regions
- PCP prescribed medium-potency TCS, but nodules and itch remained bothersome
- No coexisting atopic conditions
- Saw multiple providers and a specialist in past 2 years
CURRENT STATUS
- Medium- to high-potency TCS as needed
- Nodules remain and itch is near-constant
- Frustrated that people always tell him to stop scratching
Real image of PN.
Story inspired by people who suffer from PN.
Story inspired by people who suffer from PN.
CASE STUDY: 52-year-old female
CASE HISTORY
- Nodules developed a few months after she began experiencing itch
- Also suffers from asthma
- Medium-potency TCS provided some temporary relief
- After 1 year of frequent PCP visits, was referred to a specialist
CURRENT STATUS
- High-potency TCS daily for past 2 weeks
- Has taken 2 courses of OCS in past 6 months
- Still has widespread disease on arms and back
- People always stare, so she covers up as much skin as possible year-round
Real image of PN.
Story inspired by people who suffer from PN.
Story inspired by people who suffer from PN.
CASE STUDY: 60-year-old male
CASE HISTORY
- Itch and firm red bumps developed across body regions
- PCP prescribed medium-potency TCS, but nodules and itch remained bothersome
- No coexisting atopic conditions
- Saw multiple providers and a specialist in past 2 years
CURRENT STATUS
- Medium- to high-potency TCS as needed
- Nodules remain and itch is near-constant
- Frustrated that people always tell him to stop scratching
Real image of PN.
Story inspired by people who suffer from PN.
Story inspired by people who suffer from PN.
Is this patient ready for DUPIXENT?
Watch healthcare providers discuss when patients may be ready for DUPIXENT
OCS, oral corticosteroids; PCP, primary care physician; PN, prurigo nodularis; TCS, topical corticosteroids.