Open Up a World EXPLORE DUPIXENT DATA IN MUCUS BURDEN AND AIRWAY VOLUME1,2
See our clinical trial data below
VESTIGE: The first randomized trial to use FRI and other methods to assess the effect of DUPIXENT on FeNO, lung function, airway volume, and mucus burden
The primary imaging endpoint ([s]iVaw at TLC) did not reach statistical significance (P>0.05); therefore all subsequent endpoints are descriptive; definitive conclusions cannot be made.1
of patients were observed
to achieve FeNO <25 ppb
with DUPIXENT 300 mg Q2W + SOC
(n=72) vs 11% of placebo + SOC patients
(n=37) at Week 24 (primary endpoint)1
increase in airway volume observed
([s]iVaw at TLC) from baseline with
DUPIXENT 300 mg Q2W + SOC (n=72) vs
2% decrease with placebo + SOC (n=37)
at Week 24 (second primary endpoint)1,a
increase in pre-bronchodilator
FEV1 observed
with DUPIXENT 300 mg Q2W + SOC (n=72)
vs 270 mL with placebo + SOC (n=37) at
Week 24 (secondary endpoint)1,2,a
decrease in mucus plug score observed
with DUPIXENT 300 mg Q2W + SOC (n=72) vs
1.4 increase with placebo + SOC (n=37) (LSM
difference [SE] vs placebo: –4.9 [0.8]) at
Week 24 (secondary endpoint)1,3,a,b
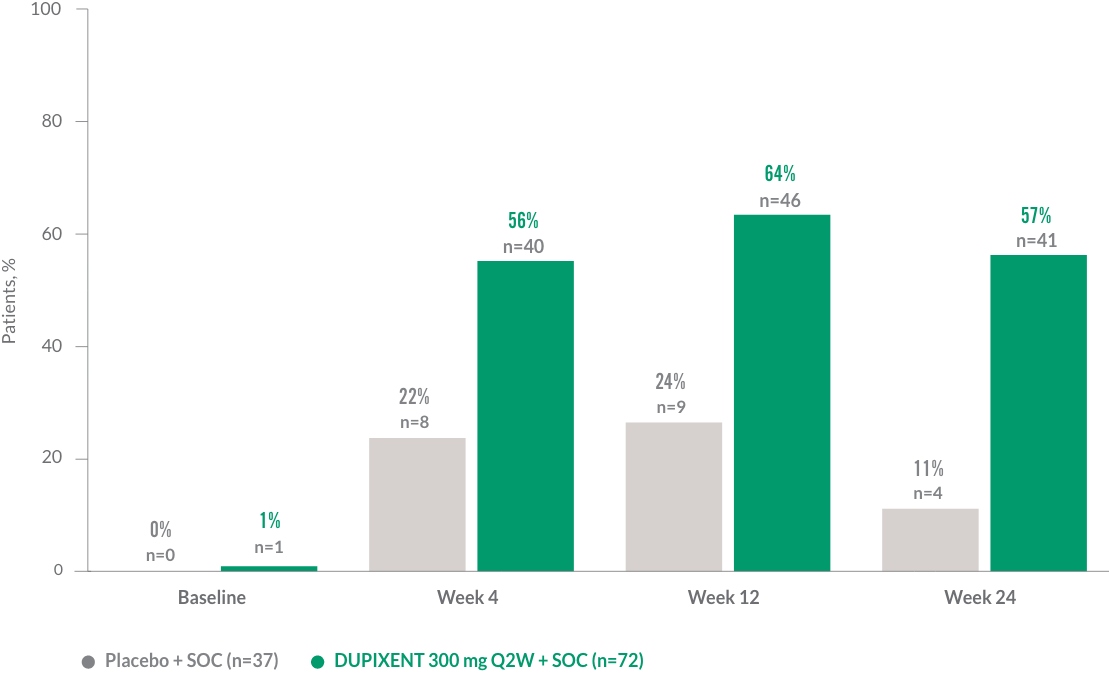
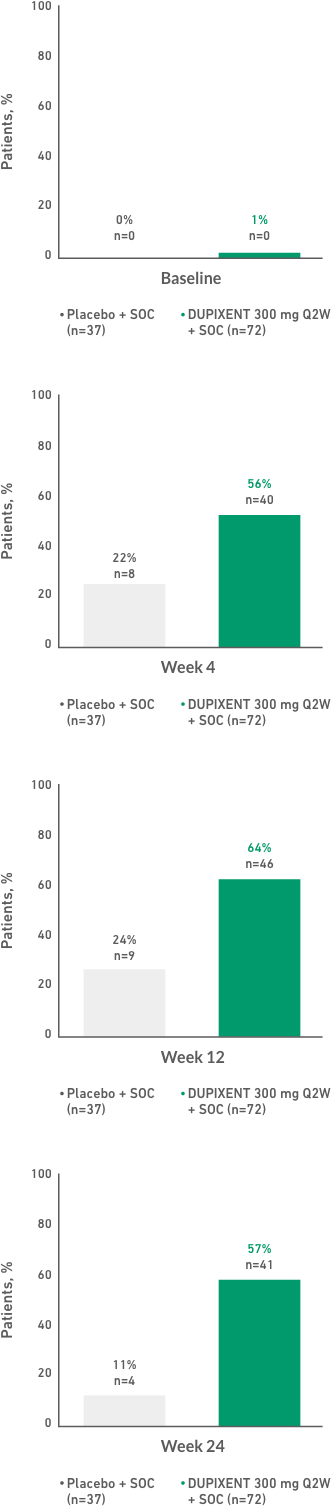
of patients were observed to reduce or eliminate mucus plugging
with DUPIXENT 300 mg Q2W + SOC (n=72) vs
a reduction in 23% of placebo + SOC patients
(n=37) at Week 24 (exploratory endpoint)1,2,a,c
aResults are descriptive. Definitive conclusions cannot be made. Please see study design for full limitations.
bThe mucus plug score was calculated as the number of bronchopulmonary segments that contained at least one mucus plug. Range was 0-18, with higher values indicating a greater mucus plug burden.1
cAt Week 24, 14.8% of DUPIXENT patients eliminated mucus plugs and 52.5% had a reduced mucus score (>0-3.5) vs 0% of placebo patients with a mucus score of 0 and 23.3% of placebo patients who had a reduced mucus score (>0-3.5).2
Decrease in mucus score with DUPIXENT was correlated with changes in pre‑
bronchodilator FEV11,d
dPearson’s correlation coefficient for mucus score/pre-bronchodilator FEV1: r[60]=−0.62.1
IL-13 signaling mediates local inflammation, impacting FeNO levels, mucus hypersecretion, and airway obstruction4,5
FeNO is a type 2 inflammation biomarker associated with exacerbation risk and lung function decline6,7
- 50% increase in exacerbation risk in patients with FeNO >50 ppb6
- 2.7 times increased risk of rapid lung function decline in patients with FeNO >40 ppb7
ONLY DUPIXENT DIRECTLY INHIBITS IL-4 AND IL-13 SIGNALING8,*
*The mechanism of dupilumab action has not been definitively established.
DUPIXENT vs 270 mL with placebo at Week 241,2


Results are descriptive. Definitive conclusions cannot be made.
Reductions in FeNO levels and increases in airway volumes were correlated with changes in lung function1,e,f
ePearson’s correlation coefficient for FeNO/pre-bronchodilator FEV1: r[68]=−0.40.1
fPearson’s correlation coefficient for (s)iVaw [%]/pre-bronchodilator FEV1: r[60]=0.23.1
(secondary endpoint, Week 24)1,b,g


Mucus plugs are defined as complete occlusions of the airway visible at TLC.
Results are descriptive. Definitive conclusions cannot be made. Change from baseline in global mucus score at Week 4 was an exploratory endpoint. Please see study design for full limitations.
gWith DUPIXENT 300 mg Q2W + SOC (n=72) vs placebo + SOC (n=37) (LSM difference [SE] vs placebo: −4.9 [0.8]).3
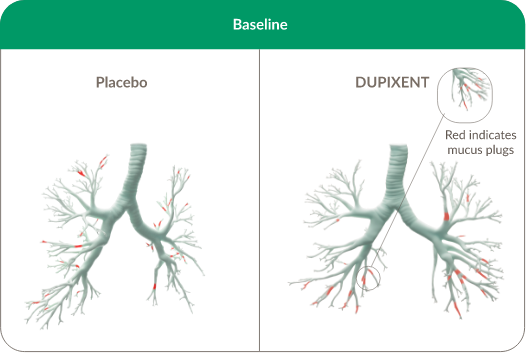
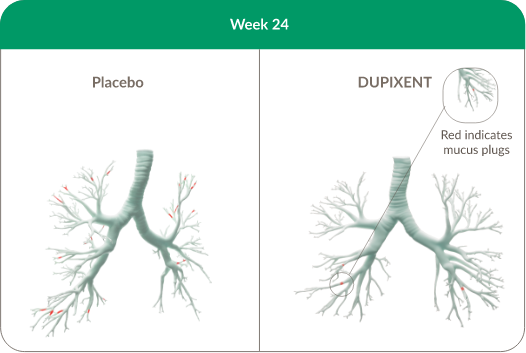
CT scans correspond to patients with changes in mucus plug volume that matched the mean percentage changes observed in the ITT population.
Results are descriptive. Definitive conclusions cannot be made.
CLINICAL TRIAL DATA
Exacerbation reduction
Up to 81% significant reduction in annualized rate of severe exacerbations through Week 24 with DUPIXENT 300 mg Q2W + SOC (n=64) vs placebo + SOC (n=68) (0.20 vs 1.04; rate ratio: 0.19 [95% CI: 0.07, 0.56]) (DRI12544, EOS ≥300 cells/μL, secondary endpoint).8
QUEST primary endpoint results (ITT population)
48% reduction in severe exacerbations at Week 52 in patients with no biomarker requirement with DUPIXENT 200 mg Q2W + SOC (n=631) vs placebo + SOC (n=317) (rate ratio: 0.52 [95% CI: 0.41, 0.66]).8,9
46% reduction in severe exacerbations at Week 52 in patients with no biomarker requirement with DUPIXENT 300 mg Q2W + SOC (n=633) vs placebo + SOC (n=321) (rate ratio: 0.54 [95% CI: 0.43, 0.68]).8,9
Lung function improvement
470 mL sustained breathing relief was seen at Week 52 from baseline in pre-bronchodilator FEV1 with DUPIXENT 200 mg Q2W + SOC (n=264) vs 170 mL with placebo + SOC (n=148) (QUEST, EOS ≥300 cells/μL, secondary endpoint).8,10,11
- 72% of the total FEV1 improvement was seen at Week 2 with DUPIXENT 200 mg Q2W + SOC (n=264) (QUEST, EOS ≥300 cells/μL, secondary endpoint)8,11
QUEST primary endpoint results (ITT population)
320 mL improvement from baseline in pre-bronchodilator FEV1 at Week 12 with DUPIXENT 200 mg Q2W + SOC (n=631) vs 180 mL with placebo + SOC (n=317) (LSM difference: 140 mL [95% CI: 80, 190 mL]).8,9
340 mL improvement from baseline in pre-bronchodilator FEV1 at Week 12 with DUPIXENT 300 mg Q2W + SOC (n=633) vs 210 mL with placebo + SOC (n=321) (LSM difference: 130 mL [95% CI: 80, 180 mL]).8,9
OCS reduction/elimination
86% of patients reduced or eliminated their OCS dose at Week 24 with DUPIXENT 300 mg Q2W + SOC (n=103) vs 68% with placebo + SOC (n=107) (VENTURE, ITT population).12
See study designs here.
CT, computed tomography; EOS, eosinophils; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; ITT, intention-to-treat; LSM, least squares mean; OCS, oral corticosteroid; Q2W, once every 2 weeks; (s)iVaw, specific image-based airway volume; SOC, standard of care; TLC, total lung capacity.