Discover helpful
resources to further
understand DUPIXENT
Watch and learn more about DUPIXENT


Dr Phipatanakul: MOD and MOA
00:00:10:15 - 00:00:41:29
Hi. My name's Wanda Phipatanakul. I'm a professor of pediatrics at Harvard Medical School. Direct the research center at Boston Children's Hospital and practice in an academic setting. During this video, we will be discussing type two inflammation and its prevalence among patients with asthma. We're going to start first by discussing uncontrolled asthma. So as you know, lots of people have asthma.
00:00:42:03 - 00:01:19:19
In fact, 25 million Americans have asthma and up to 10% of those actually require high intensity treatment to maintain control of their asthma. That can include inhaled corticosteroids in addition to other types of medications and on occasion, oral corticosteroids. Patients can have varying levels of asthma severity in many patients. Lack of symptom control can be due to underlying type two inflammation.
00:01:19:21 - 00:01:57:03
Type two inflammation is an immune response to environmental triggers such as allergens, including pollen and dust mites, among others. And when left uncontrolled, type two inflammation can result in symptoms of asthma and exacerbate other coexisting diseases such as atopic dermatitis. Chronic rhino sinusitis with nasal polyposis, and others. Up to 84% of asthma in adults is driven by type two inflammation.
00:01:57:06 - 00:02:42:25
So it's really important to think about type two inflammation in asthma. So many of these patients also rely on systemic oral corticosteroids for asthma control. Oral corticosteroids can be associated with systemic adverse effects that include obesity, type two diabetes, osteoporosis, psychological effects such as depression and anxiety, hypertension, and adrenal suppression. Even if you use oral corticosteroids in a short term, they can be associated with adverse effects, making the need to minimize oral corticosteroids use a priority.
00:02:42:27 - 00:03:20:05
Really, we should be stewards in minimizing the amount of systemic steroids that we use. Adverse effects from oral corticosteroids can be cumulative. In fact, just four lifetime births the lifetime equivalent of one gram, can significantly increase the risk of all those systemic adverse events that I spoke about. How many of your patients do you think have received four courses of oral corticosteroids over their lifetime?
00:03:20:08 - 00:03:55:22
According to recent data, more than half a million asthma patients receive two or more oral corticosteroid bursts last year. So you can imagine that these local and systemic side effects from systemic oral corticosteroids can be significant. What do we think about when patients are needing so much therapy? I think about ad on biologic therapy when a patient is really having a lot of exacerbations and they're not well controlled.
00:03:55:24 - 00:04:38:13
You think about step up therapy with a biologic per guideline recommendations. And that could be an option that could really help these patients achieve long term control of their asthma symptoms. Continue watching to learn more about type two inflammation and a biologic treatment option for appropriate asthma patients.
00:04:38:15 - 00:05:14:01
Welcome back! During this video, we will be taking an in-depth look at the path of physiology of type two inflammation. Type two inflammation is a response to the external environment that can lead to symptoms of asthma in some patients. In patients with asthma driven by underlying type two inflammation, their asthma can be more severe and present with an eosinophilic phenotype or oral corticosteroid dependance.
00:05:14:03 - 00:05:58:00
In fact, patients with underlying type two inflammation often experience symptoms as a result of a bacterial or viral infection. A trigger such as decimates or animal dander or pollen that come in contact with the airway epithelium. These patients also can present with elevated biomarkers. The current Global Initiative for Asthma or Gina guidelines define underlying type two inflammation as one or more elevated biomarker levels, including blood or sputum, eosinophil counts, and fino.
00:05:58:02 - 00:06:41:17
Gina also acknowledges that asthma patients on frequent oral corticosteroids may have underlying type two inflammation that is suppressed. So asthma, as you know, can be present alone. But many patients also have coexisting type two diseases or other comorbidities, such as chronic rhino situs situs with nasal polyposis and atopic dermatitis, which are also associated with type two inflammation. And what are some of the cytokines that are key drivers of this systemic and localized type two inflammation?
00:06:41:20 - 00:07:21:05
Two key drivers are IL for and IL 13. These cytokines bind to that shared receptor component on the IL four receptor, in which IL four and IL 13 are activated and contribute to systemic and localized inflammation. Let's start with the IL four cytokine. IL four primarily contributes to systemic type two inflammation, such as Ige production from B cells, eosinophil tracking to the site of inflammation.
00:07:21:11 - 00:08:04:25
Mast cell activation and release of inflammatory mediators and other inflammatory cytokines and processes. You also want to remember that Eosinophilic Express IL four receptor alpha complexes, which primarily signal in response to IL four, so eosinophil trafficking is also increased when activated by IL four. And you have eosinophils that just migrate to that site of inflammation. B cells also express IL four receptor alpha complexes, and they signal in response to IL four.
00:08:04:27 - 00:08:45:10
Because of this IL four signaling, the B cells undergo what we call isotype switching from IG producing cells to IG producing cells. As you know, IG is important in allergy and free Ige binds to mast cells. So if you're allergic and you have IG to specific allergens, they bind to the mast cells and basophils within the tissue. And when that IG binds to the surface of these inflammatory cells, then there's cross-linking.
00:08:45:13 - 00:09:48:19
And that signals release of inflammatory proteins such as histamine L4 and IL 13. And that in turn contributes to inflammation within the tissues. Now what about the IL 13 cytokine. I have 30 primarily contributes to localized type two inflammation. And that includes things such as mucus overproduction, broncho constriction, airway hyper responsiveness, phenol production, and epithelial barrier dysfunction. The airways also lined with structural cells, notably epithelial cells and mucus producing goblet cells, and these cells express the IL four receptor alpha complex that binds to IL four and IL 13, and these cells primarily signal in response to IL 13.
00:09:48:21 - 00:10:17:18
Now that you've seen the pathophysiology of type two inflammation, continue watching to learn more about type two inflammation and a biologic treatment option for appropriate asthma patients.
00:10:17:21 - 00:10:54:00
The mechanism of action has not been definitively established. Welcome back. During this video we will talk about Dupixent, a dual IL four and IL 13 receptor inhibitor. Dupixent is a fully human monoclonal antibody that inhibits IL four and IL 13 signaling by specifically binding to the IL four receptor alpha subunit, which is shared by both the IL four and the IL 13 receptor complexes.
00:10:54:03 - 00:11:27:10
Dupixent inhibits IL four signaling via the type one receptor, and both IL four and IL 13 signaling through the type two receptor. So type one receptors are located within the cell membranes of mass cells. Basal fills, eosinophils, neutrophils, and T cells, and type two receptors are located within the cell membranes of epithelial cells, smooth muscle cells, and fibroblasts.
00:11:27:12 - 00:12:08:17
Dupixent binds to the IL four receptor, blocking IL four and IL 13. Intracellular signaling. Pharmacodynamics. Data with Dupixent showed a decrease in total Ige and a transient increase in blood officials. Dupixent also prevents complex singing of IL 13 receptor with the IL four receptor complex. Pharmacodynamics. Data with Dupixent showed decreased phenol levels.
00:12:08:20 - 00:13:01:25
Important safety information. Continued warnings and precautions. Hypersensitivity. Hypersensitivity reactions, including anaphylaxis, serum sickness, or serum sickness like reactions. Angioedema. Generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. If a clinically significant hypersensitivity reaction occurs. Institute appropriate therapy and discontinue dupixent eosinophilic conditions. Patients being treated for asthma may present with clinical features of eosinophilic pneumonia or eosinophilic granulomatosis with polyangiitis, e.g. P.A. these events may be associated with the reduction of oral corticosteroid therapy.
00:13:01:29 - 00:13:34:17
Healthcare providers should be alert to vasculitis, rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and or neuropathy presenting in their patients with eosinophilia. Cases of eosinophilic pneumonia were reported in adults who participated in the asthma development program, and cases of Egba have been reported with Dupixent in adults who participated in the asthma development program, as well as in adults with comorbid asthma in the CRC with NP Development program.
00:13:34:18 - 00:14:08:06
Advise patients to report signs of Eocene affiliate pneumonia and consider withholding dupixent if eosinophilic pneumonia or EPA are suspected, acute symptoms of asthma or acute deteriorating disease. Do not use Dupixent to treat acute symptoms or acute exacerbations of asthma, acute bronchospasm, or status. Asthmatic patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of dupixent.
00:14:08:09 - 00:14:43:17
Risk associated with abrupt reduction of corticosteroid dosage. Do not discontinue systemic, topical or inhaled corticosteroids abruptly upon initiation of dupixent reductions, and corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a health care provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and or unmask conditions previously suppressed by systemic corticosteroid therapy.
00:14:43:20 - 00:15:18:03
Psoriasis. Cases of new onset psoriasis have been reported with the use of dupixent for the treatment of asthma, including in patients without a family history of psoriasis. In post-marketing reports, these cases resulted in partial or complete resolution of psoriasis with discontinuation of diplomat with or without use of supplemental treatment for psoriasis, topical or systemic. Those who continued to pill you received supplemental treatment for psoriasis to improve associated symptoms.
00:15:18:04 - 00:15:54:26
Advise patients to report new onset psoriasis symptoms if symptoms persist or worsen. Consider dermatologic evaluation and or discontinuation of dupixent, arthralgia, and psoriatic arthritis. Arthralgia has been reported with the use of depiction, with some patients reporting gait disturbances or decreased mobility associated with joint symptoms. Some cases resulted in hospitalization. Cases of new onset psoriatic arthritis requiring systemic treatment have been reported with the use of depictions.
00:15:55:03 - 00:16:35:27
Advise patients to report new onset or worsening joint symptoms if symptoms persist or worsen. Consider rheumatology evaluation and or discontinuation of dupixent. Parasitic helminth infections. It is unknown if dupixent will influence the immune response against helminth infections. Treat patients with preexisting helminth infections before initiating therapy with dupixent. If patients become infected while receiving treatment with Dupixent and do not respond to anti helminth treatment, discontinue treatment with Dupixent until the infection resolves.
00:16:36:04 - 00:17:20:22
Helminth infections five cases of entero biases and one case of Ascaris were reported in pediatric patients 6 to 11 years old in the Pediatric Asthma Development program. Vaccinations consider completing all age appropriate vaccinations as recommended by current immunization guidelines prior to initiating dupixent. Avoid use of live vaccines during treatment with Dupixent. Adverse reactions. The most common adverse reactions, incidence greater than or equal to 1% in patients with asthma are injection site reactions, oropharyngeal pain, and eosinophilia.
00:17:20:25 - 00:17:52:06
Use and specific populations. Pregnancy A pregnancy exposure registry monitors pregnancy outcomes in women exposed to depiction during pregnancy. Available data from case reports and case series with dupixent use and pregnant women have not identified a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Human IG antibodies are known to cross the placental barrier.
00:17:52:06 - 00:18:26:17
Therefore, dupixent may be transmitted from the mother to the developing fetus. Lactation. There are no data on the presence of dupixent in human milk. The effects on the breastfed infant or the effects on milk production. Maternal IG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered, along with the mother's clinical need for dupixent and any potential adverse effects on the breastfed child from dupixent or from the underlying maternal condition.
00:18:26:19 - 00:19:00:17
Indication dupixent is indicated as an add on maintenance treatment of adult and pediatric patients aged six years and older with moderate to severe asthma, characterized by an eosinophilic phenotype, or with oral corticosteroid dependent asthma. Limitations of use. Dupixent is not indicated for the relief of acute bronchospasm or status. Asthmatic.
00:19:00:19 - 00:19:06:05
Now that you've seen how dupixent works. Continue watching to learn more.
Dr Barberis: Asthma Patient Cases
00:00:10:23 - 00:00:30:03 I’m doctor Barberis. I work with Denver Allergy, a private practice based clinic in the Denver metro area. During this video, we're going to talk about a hypothetical patient with moderate to severe asthma with an iOS and a phenotype you might see in your practice that might benefit from Dupixent. Over the last 12 months, this patient had at least two exacerbations. 00:00:30:03 - 00:00:52:23 Despite therapy with high dose inhaled corticosteroid and long acting beta agonists. And by exacerbation, I mean she's either been seen for acute medical care, for an urgent care visit, or for an urgent visit in your office and possibly treated with oral corticosteroids. This patient really loves to hike, and due to her exacerbation, sometimes she feels like she can't fully enjoy her outdoor activities. 00:00:52:23 - 00:01:22:15 Sometimes she's nervous that she'll have symptoms while she's out on the trail. Last time she was in the Office of Full Evaluation and workup was completed, which revealed key findings. Her Act score was 18, and her pulmonary function tests revealed that her FEV one was 51% predicted, with 14% reversibility, and this concluded suboptimal control. Her bloodwork shows her most recent eosinophilic count is elevated at about 400 cells per micro leader, and after her last exacerbation, she went to see her specialist. 00:01:22:15 - 00:01:45:00 And they said, let's consider dupixent to help reduce further severe exacerbations within the need for emergency medical care. Ultimately, she was initiated under picks int she was given the first subcutaneous dose in office and trained at that time to give subsequent doses to herself at home. After a year of continued treatment with Dupixent, she's happy that she has her asthma under better control. 00:01:45:02 - 00:02:07:08 Now that you've seen a patient type that could benefit from Dupixent. Can you think of any of your own patients who might fit this profile? Continue watching to learn more about treatment with Dupixent. 00:02:07:10 - 00:02:28:23 My name is Doctor Barbera. I work with Denver Allergy, a private practice based clinic in the Denver metro area. During this video, we're going to talk about a hypothetical patient with moderate to severe asthma with an iOS and a Philip phenotype, who you might see in your practice that might benefit from dupixent. This patient has reduced lung function and persistent uncontrolled asthma. 00:02:28:24 - 00:03:00:16 In fact, at his last visit, he did a pulmonary function test which revealed that his FEV one was 58% predicted with 16% reversibility. He's using albuterol daily, along with a high dose inhaled corticosteroid and long acting beta agonist. His Act score is 16, indicating suboptimal control. His most recent blood, eosinophilic ount, is elevated at 150 cells per liter, and his final score is elevated at 35 parts per billion. 00:03:00:18 - 00:03:24:28 This patient is unable to go canoeing due to his uncontrolled asthma, because of his reduced lung function and poor asthma control. His asthma specialist is considering dupixent. This patient initiated dupixent and was given the first subcutaneous injection in office, then trained to administer dupixent at home. Now that you've seen a patient type that could benefit from treatment with Dupixent. 00:03:24:29 - 00:03:45:20 Try to think of your own patients who may be a potential candidate for dupixent based on their symptoms. Continue watching to learn more about treatment with Dupixent. 00:03:45:23 - 00:04:04:11 Hello again, I'm Doctor Barbera. I work with Denver Allergy, a private practice based clinic in the Denver metro area. During this video, we're going to talk about a hypothetical patient with oral corticosteroid dependent asthma who you may see in your practice that might benefit from dupixent. 00:04:04:14 - 00:04:33:26 Last time this patient was in the office, a full evaluation and workup was completing, which revealed key findings. His Act score was 18, and his pulmonary function tests revealed that his FEV one was 54% predicted, with 16% reversibility. This concluded suboptimal control. This patient is currently using high dose inhaled corticosteroid and long acting beta agonist, and he's also on daily maintenance oral corticosteroids to control asthma symptoms. 00:04:33:26 - 00:05:04:11 And he's concerned about the adverse effects of steroid use. He is also concerned that his weight gain may be related to consistent use of steroids. However, without the steroids, he's unable to maintain asthma control. He now avoids social activities with his friends in the city due to his symptoms and potential for frequent asthma exacerbations. Adverse effects from oral corticosteroids are cumulative over a lifetime and become significant over four lifetime births, or approximately one gram. 00:05:04:12 - 00:05:29:27 However, he has reached this amount in just the last year alone. His asthma specialist would like to consider treating him with Dupixent, since it's the only biologic indicated for oral corticosteroid dependent asthma. This patient was initiated on dupixent dosed at 300mg subcutaneous every two weeks. He was given the loading dose in office and trained at that time to administer at home. 00:05:29:29 - 00:05:45:25 After six months of treatment, he was able to reduce his oral corticosteroid dose and at the same time improved his asthma control with fewer exacerbations and improved lung function. 00:05:45:28 - 00:06:03:15 He's feeling much better and is able to get back to doing things he's enjoyed. Now that you've seen a patient type that could benefit from treatment with Dupixent. Think of some of your own patients who might also benefit. 00:06:03:17 - 00:06:56:23 Important safety information. Continued warnings and precautions. Hypersensitivity hypersensitivity reactions including anaphylaxis. Serum sickness or serum sickness like reactions. Angioedema. Generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. If a clinically significant hypersensitivity reaction occurs. Institute appropriate therapy and discontinue dupixent eosinophilic conditions. Patients being treated for asthma may present with clinical features of eosinophilic pneumonia or eosinophilic granulomatosis with polyangiitis, e.g. P.A. these events may be associated with the reduction of oral corticosteroid therapy. 00:06:56:25 - 00:07:29:11 Healthcare providers should be alert to vasculitis, rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and or neuropathy presenting in their patients with Eocene Ophelia. Cases of eosinophilic pneumonia were reported in adults who participated in the Asthma Development Program, and cases of EGP have been reported with Dupixent in adults who participated in the asthma development program, as well as in adults with comorbid asthma in the CRS with NP Development program. 00:07:29:11 - 00:08:03:04 Advise patients to report signs of iOS and affiliate pneumonia and GPA. Consider withholding Dupixent if eosinophilic pneumonia or Egba are suspected, acute symptoms of asthma or acute deteriorating disease. Do not use Dupixent to treat acute symptoms or acute exacerbations of asthma, acute bronchospasm or status. Asthmatic patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of dupixent. 00:08:03:07 - 00:08:38:14 Risk associated with abrupt reduction of corticosteroid dosage. Do not discontinue systemic, topical or inhaled corticosteroids abruptly upon initiation of dupixent. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a health care provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and or unmask conditions previously suppressed by systemic corticosteroid therapy. 00:08:38:16 - 00:09:13:01 Psoriasis. Cases of new onset psoriasis have been reported with the use of depictions for the treatment of asthma, including in patients without a family history of psoriasis. In post-marketing reports. These cases resulted in partial or complete resolution of psoriasis, with discontinuation of diplomat with or without use of supplemental treatment for psoriasis, topical or systemic. Those who continued to pill Umar received supplemental treatment for psoriasis to improve associated symptoms. 00:09:13:02 - 00:09:57:18 Advise patients to report new onset psoriasis symptoms if symptoms persist or worsen. Consider dermatologic evaluation and or discontinuation of dupixent, arthralgia and psoriatic arthritis. Arthralgia has been reported with the use of depictions, with some patients reporting gait disturbances or decreased mobility associated with joint symptoms. Some cases resulted in hospitalization. Cases of new onset psoriatic arthritis requiring systemic treatment have been reported with the use of depiction advise patients to report new onset or worsening joint symptoms if symptoms persist or worsen. 00:09:57:18 - 00:10:44:05 Consider rheumatology evaluation and or discontinuation of dupixent. Parasitic helminth infections. It is unknown if dupixent will influence the immune response against helminth infections. Treat patients with preexisting helminth infections before initiating therapy with dupixent. If patients become infected while receiving treatment with Dupixent and do not respond to anti helminth treatment, discontinue treatment with Dupixent until the infection resolves. Helminth infections five cases of entero biases and one case of Ascaris were reported in pediatric patients 6 to 11 years old in the Pediatric Asthma Development program. 00:10:44:08 - 00:11:27:23 Vaccinations consider completing all age appropriate vaccinations as recommended by current immunization guidelines prior to initiating dupixent. Avoid use of live vaccines during treatment with Dupixent. Adverse reactions. The most common adverse reactions incidence greater than or equal to 1% in patients with asthma are injection site reactions, oropharyngeal pain and eosinophilia. Use and specific populations. Pregnancy A pregnancy exposure registry monitors pregnancy outcomes in women exposed to depiction during pregnancy. 00:11:27:26 - 00:12:02:13 Available data from case reports and case series with dupixent use, and pregnant women have not identified a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Human IG antibodies are known to cross the placental barrier. Therefore, dupixent may be transmitted from the mother to the developing fetus. Lactation. There are no data on the presence of dupixent in human milk, the effects on the breastfed infant, or the effects on milk production. 00:12:02:16 - 00:12:40:11 Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered, along with the mother's clinical need for dupixent and any potential adverse effects on the breastfed child from dupixent or from the underlying maternal condition. Indication dupixent is indicated as an add on maintenance treatment of adult and pediatric patients aged six years and older with moderate to severe asthma, characterized by an eosinophilic phenotype, or with oral corticosteroid dependent asthma. 00:12:40:14 - 00:12:51:02 Limitations of use. Dupixent is not indicated for the relief of acute bronchospasm or status asthmatic. 00:12:51:04 - 00:12:54:07 Continue watching to learn more about treatment with dupixent.Dr Fussel: DUPIXENT Clinical Trial Data
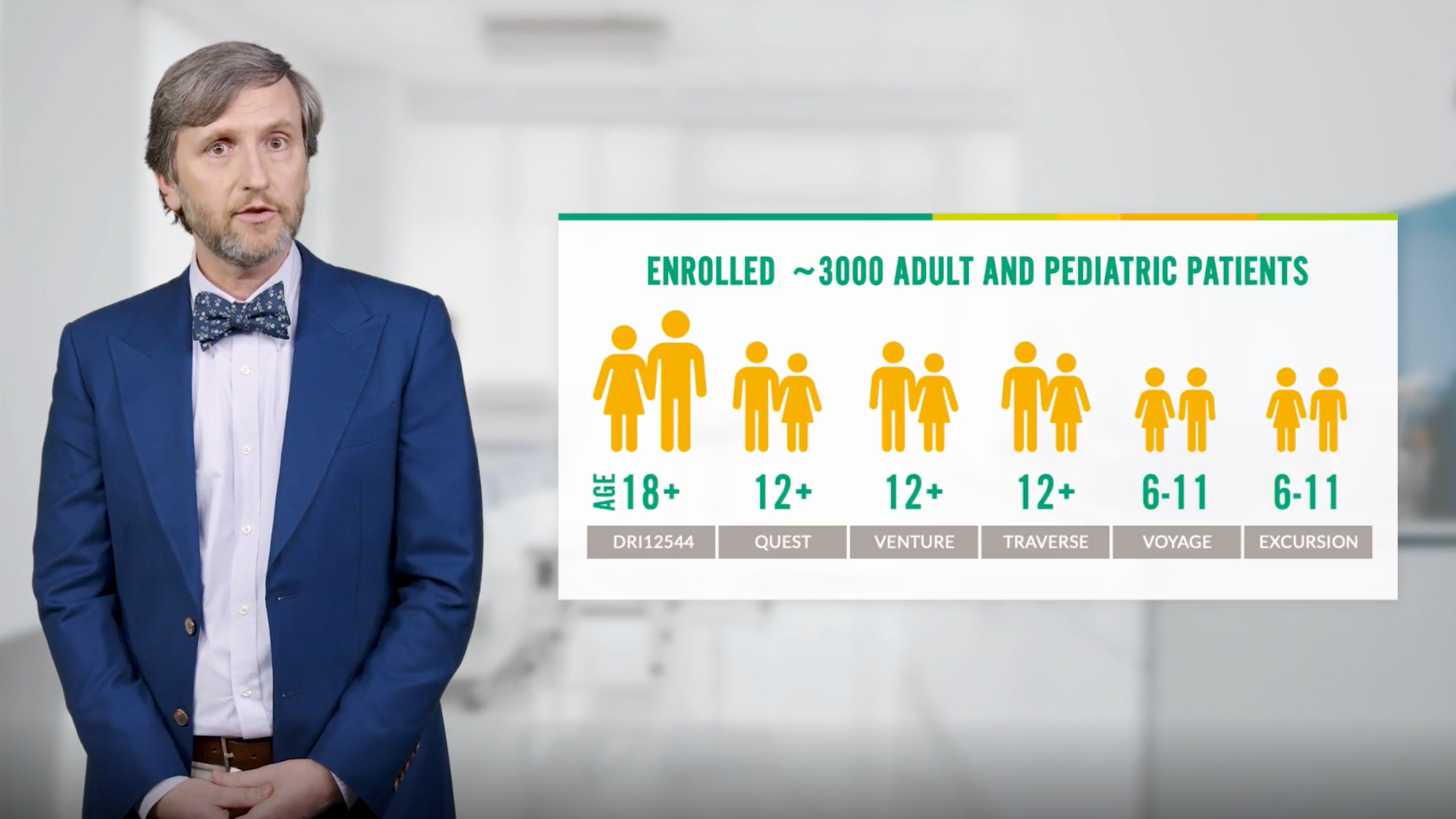
00;00;10;11 - 00;00;38;00 Hello. My name is Kevin. I'm a pulmonary critical care physician with Coastal Pulmonary Associates in Encinas, California. During this video, we're going to talk about the clinical trials from the Dupixent Asthma Clinical Development Program. The Dupixent Asthma Clinical Development program enrolled approximately 3000 pediatric adolescent and adult patients with asthma, including patients treated for up to three years. Let's discuss these trials in the phase two B study. 00;00;38;01 - 00;01;17;12 Dry 12544 patients on a medium or high dose inhaled Corrigan steroid or ICS in a long acting beta agonist or larva were enrolled without a biomarker requirement and randomized to dupixent 300mg or 200mg or placebo every two weeks for a 24 week treatment period. In quest of phase three study, patients on a medium or high dose ICS plus up to two additional controllers and bloodiest infos, less than 1500 cells per Micro Leader were randomized to either Dupixent 300mg or 200mg every two weeks, or match placebo for 52 weeks. 00;01;17;15 - 00;01;49;14 About half the patients enrolled in these two trials had one exacerbation in the year before enrollment. Additionally, about half of the enrolled patients were taking medium dose ICS plus up to two additional controllers, such as Alaba. The oral corticosteroid or ox sparing effect of dupixent was studied in venture, a phase 324 week study. Patients who required daily OCS, high dose ICS, at least one and up to two additional controllers and had blood is in a foes less than 1500 cells per micro liter or randomized. 00;01;49;14 - 00;02;25;09 It depicts 300mg or placebo. After a period of OCS dose stabilization, patients underwent timed OCS reductions. They could reduce their OCS dose as long as asthma control was maintained. During the last four weeks of the treatment period, patients maintained the lowest OCS dose achieved during the reduction phase in the year prior to the study. While a subset of patients did not have exacerbations, most patients had at least two exacerbations despite maintenance OCS, in addition to patients being on an average of 11mg of daily OCS, all were on additional asthma controllers. 00;02;25;16 - 00;02;54;01 High dose ICS was a requirement for enrollment. Additionally, just over half of patients were on three asthma controllers, including the required high dose ICS, a lava, and a long acting muscarinic receptor antagonist, Lama. The mean baseline blood is count was 350 cells per milliliter. However, the majority of patients had less than 300 cells per milliliter. AD enrollment OCS can affect biomarker levels, including bloodiest cinephiles. 00;02;54;03 - 00;03;24;10 Patients who completed the phase tube study, Dry 12544, Quest and Venture were given the option to enroll and traverse a 96 week open label extension study. In traverse. All patients were taking Dupixent 300mg every two weeks. For patients with ox dependent asthma. OCS reductions were made at the discretion of the treating physician. The primary endpoint of traverse was the number and percentage of patients having any treatment emergent adverse event up to week 96. 00;03;24;13 - 00;03;49;26 Now we will discuss the safety profile, adverse reactions occurring in greater than or equal to 1% of patients treated with depiction, and at a higher rate than placebo in the phase two be studied dry one, two, five, four, four and quest were injection site reactions, oral pharyngeal pain and defined as bloodiest and officials greater than 3000 cells per liter or deemed by the investigator to be an adverse reaction. 00;03;50;00 - 00;04;32;23 None met the criteria for serious iOS and conditions. Adverse reactions occurring in greater than or equal to 5% of patients in either group in venture included viral, upper respiratory tract infection, bronchitis, sinusitis, influenza, eosinophilia, injection site reaction, and greater than or equal to one measurement of blood count greater than 3000 cells per milliliter in the traverse open label extension study, the most frequently reported treatment emergent adverse events occurring in greater than or equal to 10% of patients were nasal pharyngitis, bronchitis, upper respiratory tract infection, influenza, pharyngitis, headache, injection site erythema, and injection site pyrites. 00;04;32;27 - 00;05;03;24 For more information, please see additional important safety information throughout and at the end of this video. Now that you have viewed information regarding the Dupixent Clinical Development program, continue watching to learn more. 00;05;03;27 - 00;05;31;16 Hello, my name is Kevin. I'm a pulmonary critical care physician with Coastal Pulmonary Associates in Encinitas, California. During this video, we're going to talk about specific clinical trial data related to dupixent and asthma exacerbations in the phase two B study. Dry 1254 for treatment with dupixent. Reduced exacerbations in patients with blood essentials greater than or equal to 300 cells per micro liter through week 24. 00;05;31;19 - 00;05;58;16 This is a secondary endpoint. Quest met the coprime endpoint of annualized rate of severe exacerbations in the overall study population. As a physician, a primary goal for my patients is to avoid hospitalizations and the need for emergency care. In traverse, 97% of patients did not have an asthma exacerbation requiring hospitalization or emergency department visit. Traverse open label extension study results are descriptive. 00;05;58;17 - 00;06;26;14 Definitive conclusions cannot be made. Data were not multiplicity controlled, and there are limitations associated with open label study design, including lack of a comparator arm, decreasing sample size and potential, continued involvement of responders, and attrition of non responders. Additionally, 89% of patients had zero exacerbations during year three of six. In treatment, 74% of patients rolled over from both the phase two B study. 00;06;26;16 - 00;06;58;19 Dry 12544 in quest had no exacerbations over almost three years of treatment. Now we will discuss the safety profile. Adverse reactions occurring in greater than or equal to 1% of patients treated with Dupixent and at a higher rate than placebo in the phase two B study. Dry 12544 and quest or injection site reactions. Oral pharyngeal pain and the is defined as bloodiest and fills greater than 3000 cells per liter or deemed by the investigator to be an adverse reaction. 00;06;58;21 - 00;07;27;19 None of the criteria for serious is and conditions. Now that we reviewed exacerbation reductions with Dupixent. Continue watching to learn more. 00;07;27;22 - 00;07;52;15 Hello, my name is Kevin Fussell. I'm a pulmonary critical care physician with Coastal Pulmonary Associates in Encinitas, California. During this video, we're going to talk about specific clinical trial data related to dupixent and lung function. Quest met the coprime endpoint of change from baseline in pre bronchodilator forced expiratory volume in one second or five one at week 12, in the overall population. 00;07;52;20 - 00;08;14;20 This graph shows the five one improvement of Dupixent 200mg versus placebo in the population of patients with bloodiest in A fills greater than or equal to 300 cells per micro liter over 52 weeks in quest, most of the lung function improvement would depicts it was seen as early as week two after the first dose. Lung function improvements were sustained over one year. 00;08;14;22 - 00;08;43;27 Lung function improvements reported in traverse were sustained up to three years. This was demonstrated by patients who were initially enrolled to either dupixent or placebo. Inquest. One of the parent studies, an improvement of 100 to 200ml, can be considered clinically meaningful improvement in lung function. Now we will discuss the safety profile. Adverse reactions occurring in greater than or equal to 1% of patients treated with Dupixent and at a higher rate than placebo in the phase two B study. 00;08;44;00 - 00;09;26;06 Dry one, two, five, four, four and quest were injection site reactions, oral pharyngeal pain, and the acid defined as bloodiest and fills greater than 3000 cells per milliliter or deemed by the investigator to be an adverse reaction. None met the criteria for serious eosinophilic conditions. Now that we've reviewed lung function improvement with Dupixent, continue watching to learn more. 00;09;26;08 - 00;09;54;16 Hello, my name is Kevin Fussell. I'm a pulmonary critical care physician with Coastal Pulmonary Associates and Encinitas, California. During this video, we're going to talk about specific clinical trial data related to dupixent and oral corticosteroid or Oxus. Did you know that just for lifetime bursts of OCS equivalent to 0.5 to 1g can lead to adverse effects? Add on low dose OCS or sometimes prescribed as maintenance therapy. 00;09;54;18 - 00;10;29;06 However, guidelines state that maintenance OCS should be used as a last resort treatment option for patients with asthma and venture patients taking Dupixent 300mg plus danger of care experience a 70% mean 100% median dose reduction of their daily OCS dose from baseline at week 24, which was the primary endpoint. Secondary endpoints in venture demonstrated that patients were able to reduce or eliminate the rocks dose, while simultaneously reducing the rate of severe exacerbations and improving their lung function. 00;10;29;08 - 00;11;02;09 In traverses secondary endpoints, 89% of OCS dependent patients were able to reduce their OCS dose, while 79% were able to eliminate the rocks dose at week 96. Traverse open label extension results are descriptive. Definitive conclusions cannot be made. Data were not multiplicity controlled, and there are limitations associated with open label study design, including lack of a comparator arm, decreasing sample size and potential, continued involvement of responders, and attrition of non responders. 00;11;02;12 - 00;11;35;29 Now we will discuss the safety profile. The most common adverse reactions occurring in greater than or equal to 5% of patients in venture included viral, upper respiratory tract infection, bronchitis, sinusitis, influenza, eosinophilia, injection site reaction, and greater than or equal to one. Measurement of blood count greater than 3000 cells per micro leader. Now that we have reviewed the Ox sparing data with Dupixent, continue watching for additional important safety information. 00;11;36;01 - 00;12;29;09 Important safety information. Continued warnings and precautions. Hypersensitivity. Hypersensitivity reactions, including anaphylaxis, serum sickness or serum sickness like reactions. Angioedema, generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported if a clinically significant hypersensitivity reaction occurs. Institute appropriate therapy and discontinue dupixent eosinophilic conditions. Patients being treated for asthma may present with clinical features of Eocene affiliate pneumonia or eosinophilic granulomatosis with polyangiitis, e.g., these events may be associated with the reduction of oral corticosteroid therapy. 00;12;29;12 - 00;13;02;02 Healthcare providers should be alert to vasculitis, rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and or neuropathy presenting in their patients with eosinophilia. Cases of Eocene affiliate pneumonia were reported in adults who participated in the Asthma Development Program, and cases of EPA have been reported with Dupixent in adults who participated in the asthma development program, as well as in adults with comorbid asthma in the CRC with NP Development program. 00;13;02;04 - 00;13;35;22 Advise patients to report signs of Is an affiliate pneumonia and EPA consider withholding dupixent if eosinophilic pneumonia or are suspected acute symptoms of asthma or acute deteriorating disease. Do not use dupixent to treat acute symptoms or acute exacerbations of asthma, acute bronchospasm or status. Asthmatic patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of dupixent. 00;13;35;24 - 00;14;11;04 Risk associated with abrupt reduction of corticosteroid dosage. Do not discontinue systemic, topical or inhaled corticosteroids abruptly upon initiation of dupixent reductions, and corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a health care provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and or unmask conditions previously suppressed by systemic corticosteroid therapy. 00;14;11;06 - 00;14;45;21 Psoriasis. Cases of new onset psoriasis have been reported with the use of depictions for the treatment of asthma, including in patients without a family history of psoriasis. In post-marketing reports, these cases resulted in partial or complete resolution of psoriasis with discontinuation of diplomat with or without use of supplemental treatment for psoriasis. Topical or systemic. Those who continued deployment received supplemental treatment for psoriasis to improve associated symptoms. 00;14;45;22 - 00;15;22;15 Advise patients to report new onset psoriasis symptoms if symptoms persist or worsen, consider dermatologic evaluation and or discontinuation of dupixent, arthralgia, and psoriatic arthritis. Arthralgia has been reported with the use of depressant, with some patients reporting gait disturbances or decreased mobility associated with joint symptoms. Some cases resulted in hospitalization. Cases of new onset psoriatic arthritis requiring systemic treatment have been reported with the use of depictions. 00;15;22;23 - 00;16;03;19 Advise patients to report new onset or worsening joint symptoms if symptoms persist or worsen. Consider rheumatology evaluation and or discontinuation of dupixent. Parasitic helminth infections. It is unknown if dupixent will influence the immune response against helminth infections. Treat patients with preexisting helminth infections before initiating therapy with dupixent. If patients become infected while receiving treatment with Dupixent and do not respond to anti-human treatment, discontinue treatment with Dupixent until the infection resolves. 00;16;03;25 - 00;16;51;06 Helminth infections five cases of entero biases and one case of Ascaris were reported in pediatric patients 6 to 11 years old in the Pediatric Asthma Development program. Vaccinations consider completing all age appropriate vaccinations as recommended by current immunization guidelines prior to initiating dupixent. Avoid use of live vaccines during treatment with Dupixent. Adverse reactions. The most common adverse reactions incidence greater than or equal to 1% in patients with asthma are injection site reactions, oropharyngeal pain, and eosinophilia use and specific populations. 00;16;51;14 - 00;17;25;17 Pregnancy A pregnancy exposure registry monitors pregnancy outcomes in women exposed to depiction during pregnancy. Available data from case reports and case series with dupixent use and pregnant women have not identified a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier. Therefore, dupixent may be transmitted from the mother to the developing fetus. 00;17;25;19 - 00;17;54;10 Lactation. There are no data on the presence of dupixent in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered, along with the mother's clinical need for dupixent and any potential adverse effects on the breastfed child from dupixent or from the underlying maternal condition. 00;17;54;12 - 00;18;21;24 Indication dupixent is indicated as an add on maintenance treatment of adult and pediatric patients aged six years and older with moderate to severe asthma, characterized by an Eocene affiliate phenotype, or with oral corticosteroid dependent asthma. Limitations of use. Dupixent is not indicated for the relief of acute bronchospasm or status asthmatic.Mark your calendars for these future events to learn more
American College of Chest
Physicians 2026
October 2026
American College of Allergy,
Asthma & Immunology
(ACAAI) 2026
November 2026
Consider partnering with a pulmonologist or allergist to identify patients appropriate for DUPIXENT

Help eligible patients start and stay on track with DUPIXENT
DUPIXENT MyWay is a patient support program that offers insurance coverage support, financial assistance, and resources to help eligible patients who are prescribed DUPIXENT.
WATCH INFORMATIONAL
VIDEOS ABOUT:
Contact a Field Representative
Connect with a DUPIXENT Field Representative to get answers to your product-related questions and to request samples.